
Research Article / Open Access
DOI:10.31488/bjg.1000135
Quality of Colonoscopies Under Kalinox during the COVID-19 Epidemic
Rim Abboud*1,2 ,Guy Houist2, Benedicte Lambare 2
1. Gastroenterology and Hepatology, Lebanese University Faculty of Medicine, BEIRUT, LBN
2. Gastroenterology and Hepatology, Centre Hospitalier Sud Francilien, Corbeil-Essonnes, FRA
*Corresponding author: Rim Abboud, Gastroenterology and Hepatology, Lebanese University Faculty of Medicine, BEIRUT, LBN
Abstract
Colonoscopy is a major procedure for the screening and diagnosis of colorectal lesions. In France, general anesthesia remains the most widely used sedation method for colonoscopy. Faced with several constraints, other methods of sedation have been adopted. The best known is sedation by equimolar mixture of oxygen and nitrous oxide (MEOPA) marketed under the name of Kalinox, and which is offered as a second intention after general anesthesia. Since March 2020, the health crisis caused by COVID-19 has forced us to offer colonoscopy under Kalinox to patients who, before the crisis, could have benefited from general anesthesia. We present a monocentric retrospective study at the southern Ile de France hospital center (CHSF), the aim of which is to assess the quality of colonoscopies performed under Kalinox in the first line. Between 01/01/2019 and 05/31/2021 inclusive, 9 doctors with different experience performed 284 colonoscopies under Kalinox at the CHSF. The first group included 65 colonoscopies over 15 months before the COVID-19 health crisis, i.e. from January 2019 to March 2020 inclusive and the second group included 217 colonoscopies over 14 months during COVID-19, i.e. between April 2020 and May 2021 inclusive. We studied the epidemiological characteristics of the patients (gender, age), the quality of the preparation according to the Boston Bowel Preparation Scale (BBPS), the cecal intubation rate (CIR), adenoma detection rate (ADR), polyp detection rate (PDR), cancer detection rate (CDR), and the complications. The main criterion was the percentage of complete colonoscopies and the secondary criteria were: ADR, PDR, and CDR. We concluded that the KALINOX enabled us to continue screening for colorectal cancer with acceptable CIR and ADR. This simpler and less expensive method of sedation should be offered to a greater number of patients.
Keywords: gastroenterology, colonoscopy, colorectal cancer, anesthesia, kalinox. covid-19
Introduction
In France, colorectal cancer ranks third in terms of prevalence. Each year, it affects more than 45,000 people and results in 18,000 fatalities [1]. The incidence and mortality of colorectal cancer are decreased through screening. In a directive from December 2003, the European Commission recommended a two-step screening technique based on doing Fecal Immunological Test (FIT) in individuals aged 50 to 74 who are asymptomatic and at moderate risk of colon cancer every two years. Patients with positive FIT and those with a high risk of colon cancer should get a colonoscopy right away [2]. For colonoscopy, many anesthetic techniques areemployed. The method of sedation that is most frequently utilized is general anesthesia.
Due to a number of restrictions, including the difficulty of accessing the operating room, the length of the hospital stays, and the contraindications to general anesthesia, numerous sedation techniques have been adopted, the most well-known is sedation by MEOPA, which is marketed under the trade name Kalinox and given as a secondary goal after general anesthesia. France has authorized MEOPA since August 27, 2003. It is a gas made up of a mixture of 50% nitrous oxide and 50% oxygen. It works through inhalation, lowering the threshold of pain perception while producing an analgesic effect. As a result, aware sedation is produced.
A facial mask that has been adjusted to the morphology can be used for self-administration of the MEOPA. The patient breathes normally during the time of the gesture. The nurse maintains verbal control with the patient throughout the administration. Adverse effects are rare (euphoria, sedation, dizziness, nausea, anxiety) and disappear as soon as inhalation is stopped [3]. A number of earlier studies have demonstrated that colonoscopies performed under Kalinox are equally safe and effective as those performed under intravenous conscious sedation [4-6]. In France Vidal Alain et al., studied the feasibility of colonoscopies with analgesia by Kalinox from 04/12/2003 to 14/10/2004, 77 colonoscopies were performed by the same operator in the same center. Excluding organic stenoses, colonoscopy was complete in 90% of cases and 54/59 patients would accept colonoscopy under the same conditions [7]. Clara Beunon et al., conducted a study in 2021 to evaluate colonoscopies performed under Kalinox. The results of this cohort showed that this examination is feasible in routine practice with acceptable success rates in the event of a pandemic [8]. However, when Lamarque et al., conducted a prospective, multi-centric, randomized study to compare the acceptability and tolerance of colonoscopy on Kalinox versus general anesthesia, they discovered that sedation with Kalinox is not a practical substitute for general anesthesia for the practice of colonoscopy [9]. Because COVID-19 restricted access to the operating room, we had to provide colonoscopies on Kalinox to patients who would have received general anesthesia before the crisis. We performed a retrospective single-center study to evaluate the efficacy of Kalinox-treated colonoscopies during the COVID-19 pandemic.
Materials and Methods
Study design
This is a retrospective study that was conducted at CHSF. The data was collected from medical records and hospital reports of patients: paper and REFERENCE software within the Hospital. Data was saved pseudo-anonymously in a password-protected Excel spreadsheet hosted on the hospital network. It included all adult patients who underwent a colonoscopy under Kalinox at the CHSF from 01/01/2019 to 05/31/2021. Non-adult patients were excluded. Colonoscopy under general anesthesia was excluded. An ethical opinion was requested from the Ethics Committee of the CHSF. It has been approved with an approval number NCT05336617. An information letter was sent to eligible patients before their inclusion. If there was no response within 30 days, the patient was considered to be in favor of inclusion in the study.
Procedure
Nine physicians with varying levels of experience performed the colonoscopies. Two nurses were in the endoscopy room, one of whom was responsible for holding the Kalinox mask and communicating with the patient during the examination.
Variables measured
We studied the BBPS and we divided it into 3 categories: good (BBPS 7,8,9), poor (BBPS 4,5,6) and unsatisfactory (BBPS 1,2,3), CIR, PDR, ADR, and CDR.
Statistical analyzes
Statistical analysis was performed using the statistical software Statistical Package for Social Sciences (SPSS), version 22.0. Descriptive statistics were reported using means and standard deviations (SD) for continuous variables and frequency with percentages for categorical variables. We assessed differences between the two groups using the two-sample t-test for continuous variables and Pearson's chi-square or Fisher's exact test for categorical variables. All tests were two-sided, with a significance level of P value < 0.05.
Results
Demographics
Table 1 illustrates the demographics of the study participants. Of the 284 patients who met the inclusion criteria, two declined participation in the study. A total of 282 patients took part in the study, of whom 107 (37.9%) were male and 175 (62.1%) were female. The age of study participants varied between 30 and 93 years, with an average of 69.7 years and a standard deviation of 13.6. The study sample was divided into 2 groups: Group 1 included patients enrolled during the period from January to March 2019, Group 2 included patients enrolled between April 20 19 and May 2021. Age and gender did not reveal any statistically significant differences between the two study groups (P-value 0.05).
Table 1Demographic characteristics of the study participants
| Variables | All (N=282) | Group 1 Jan 2019-March 2019 (n=65) |
Group 2 April 2019- May 2021 (n=217) |
P-value |
|---|---|---|---|---|
| Age (Mean ±SD) | 69.7±13.6 | 71±14.9 | 69.2±13.2 | 0.248 |
| Age group n (%) | 0.333 | |||
| ≤65 years | 101(35.6) | 20 (30.8) | 81(37.3) | |
| >65 | 183(64.4) | 45(69.2) | 136(62.7) | |
| Gender n (%) | 0.847 | |||
| Male | 107(37.9) | 41(63.1) | 134(61.8) | |
| Female | 175(62.1) | 24(36.9) | 83(38.2) |
n frequency, SD Standard deviation, % percentage, P-value less than 0.05 is considered significant
BBPS
Bowel preparation was rated as good (BBPS 7, 8 & 9), poor (BBPS 4.5 & 6), and unsatisfactory (BBPS 1.2 & 3) in 53 (81.5%), 9 (13.8 %) and 3 (4.6%) patients in Group 1, respectively, and 167 (77.7%), 39 (18.1%) and 9 (4.2%) in Group 2 patients respectively. No significant difference was found in the quality of bowel preparation between the two groups (P-value = 0.778).
CIR
Table 2 presents the CIRs between the 2 groups and within the two groups stratified by gender, age group and BBPS. The CIR was 64.6% (42/65) in Group 1 and 76.9% (166/217) in Group 2 (P-value = 0.054). The results also showed that the CIR was higher in male than in female in Group 1 (31 [75.6%] male versus 11 [45.8%] female), but there was no significant difference between genders in Group 2 (P value = 0.079) [Table 2]. The CIR was higher in female in Group 2 (59 [71.1%]) than in their counterparts in Group 1 (11 [45.8%]) (P value = 0.029). Age group analysis showed that the CIR was higher (70 [87.5%]) in patient’s younger than 65, compared to patients 65 or older (96 [70, 6%]) (P-value = 0.004). However, there was no significant difference between the two groups (P-value = 0.243) in Group 1. Results also showed that CIR didn’t differ between the three BBPS categories. However, in Group 2 results revealed a significant difference between the three categories with 22.2%, 66.7% and 83.1% in unsatisfactory, poor and good BBPS categories respectively. Moreover, between groups a significant difference was revealed between the good categories of the BBPS (P-value= 0.011).
Table 2. Cecal intubation rate between the 2 groups and within the 2 groups stratified by gender, age group and n frequency, % percentage, CIR Cecal intubation rate, BBPS Boston Bowel Preparation Scale, P-value less than 0.05 is considered significant.
| Variables | Group 1 Jan 2019-March 2019 (n=65) |
Group 2 April 2019- May 2021 (n=217) |
P-value |
|---|---|---|---|
| CIR n (%) | |||
| All sample | 42(64.6) | 166(76.9) | 0.054 |
| CIR by Gender | |||
| Female | 11(45.8) | 59(71.1) | 0.029 |
| Male | 31(75.6) | 107(80.7) | 0.513 |
| P-value | 0.015 | 0.079 | |
| CIR by Age category | |||
| Age ≤ 65 years | 15(75.0) | 70(87.5) | 0.292 |
| Age >65 years | 27(60.0) | 96(70.6) | 0.201 |
| P-value | 0.243 | 0.004 | |
| CIR by BBPS | |||
| Unsatisfactory | 2(66.7) | 2(22.2) | 0.236 |
| Poor | 5(55.6) | 26(66.7) | 0.701 |
| Good | 35(66.0) | 138(83.1) | 0.011 |
| P-value | 0.829 | < 0.0001 |
ADR, PDR and CDR
Table 3 shows the ADR, PDR, and CDR between the study groups. ADR was 21.5% in Group 1 compared with 24.4% in Group 2. PDR was 35.4% in Group 1 compared to 33.2% in Group 2. Group 1 CDR (10.8%) was almost twice as high as Group 2 (5.5%). The results showed no significant difference in ADR, PDR and CDR between the 2 groups.
Table 3.Adenoma, polyp and cancer detection rate between the study groups
| Variables | Group 1 Jan 2019-March 2019 (n=65) | Group 2 April 2019- May 2021 (n=217) | P-value |
|---|---|---|---|
| ADR | 14(21.5) | 53(24.4) | 0.740 |
| PDR | 23(35.4) | 72(33.2) | 0.766 |
| CDR | 7(10.8) | 12(5.5) | 0.159 |
n frequency, % percentage, P-value less than 0.05 is considered significant
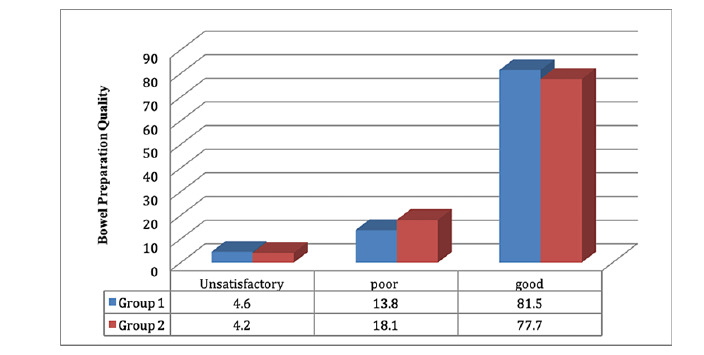
Figure 1.Bowel preparation quality between the 2 groups of the study
Discussion
The preferred type of sedation during a colonoscopy is general anesthesia. In an unusual circumstance, Kalinox sedation was administered to practically all patients during the COVID-19 public health emergency. The outcomes were satisfactory and on par with Kalinox sedation, which is typically used for elderly patients or people who cannot safely undergo general anesthesia. The median age of the 282 patients included in this study, 107 male and 175 female, was 69.7 years. The patients were split into two groups: the first group included patients who were treated over a 15-month period prior to COVID-19, and the second group included patients who were treated within 14 months of the COVID-19 crisis. Age and gender differences between the two groups were statistically insignificant. Without statistical significance, 81.5% of group 1 and 77.7% of group 2 had adequate colonic preparation. This might be as a result of the patients receiving clear instructions on dosage and administration before to colonoscopy, as well as the nurses' and doctors' stress on the necessity of the preparation.
Primary endpoint
The primary endpoint was the percentage of complete colonoscopy. The percentage of complete colonoscopies must be at least 90% and should eventually tend towards 95% [1]. We note that the CIR was 73.7% in all samples. In Group 1 was 64.4% lower than in Group 2 which was 76.9%. Before the COVID-19 epidemic, the choice of Kalinox was limited to the most fragile patients (from a health perspective), the percentage of complete colonoscopies was slightly lower but not significant. During a health crisis, in Group 2, when Kalinox was offered to all patients, some of whom could have benefited from general anesthesia in normal times, the results were comparable to Group 1. This increase in the number of colonoscopies under KALINOX enabled us to continue screening for colorectal cancer and to avoid a loss of opportunity for our patients. We stratified the CIR by age. There was no significant difference between the two age groups (P-value = 0.243) in Group 1. However, in Group 2, the CIR was higher (70 [87.5%]) in patients less than 65 years old, compared to patients who were 65 years old or older (96 [70.6%]) (P value = 0.004). In our opinion, this is related to the ability of young patients to hear the nurse's advice well and to synchronize their breathing well and to better tolerate the MEOPA mask which allows the endoscopist to complete the colonoscopy, as well as to the aging process. which takes place in the colon [10]. When we stratified the CIR by gender, we found that the CIR was higher in men than in women in Group 1 (31 [75.6%] male versus 11 [45.8%] female), but there was no significant gender difference in Group 2 (P value = 0.079) [Table 2]. This is similar to other studies where lower CIRs were seen in women [11-13]. One explanation for this gender difference is that females have been reported to have longer and more sharply angular colons than males [14]. Using the BBPS score, the preparation was evaluated. The 2009-created BBPS is a 10-point scale that evaluates bowel preparation following the conclusion of all cleansing techniques [15]. The measure ranks each segment of the colon on a scale from 0 to 3. Based on the sum of these ratings, a final score ranging from 0 to 9 is produced, with a higher number indicating more mucosa is visible. The BBPS score did not significantly differ between Groups 1 and 2 (P-value = 0.749). This was expected because both groups adhered to the same colonic preparation protocol. However, Group 2's results showed a large CIR difference, with 22.2% in the category classified as unsatisfactory, 66.7% in the bad category, and 83.1% in the good preparation category. These results are very similar to those in the literature where suboptimal bowel preparation was found to prolong overall procedure time and decrease cecal intubation rate [16].
Secondary endpoints
The effectiveness of colonoscopy to reduce CRC risk is dependent on the ability of the endoscopist to detect and remove adenomatous polyps. Corley DA, et al., demonstrated that 1% of the additional ADR reduces the risk of colorectal cancer by 3% [17]. The ADR of the endoscopist is at present the "standard of excellence" for quality measurements in screening colonoscopy. As a result, it has previously been advised that each endoscopist should find one or more adenomas in at least 25% of men and 15% of women who receive screening colonoscopies and are under the age of 50 [18]. In our study the ADR for the population was 24.3 %, the CDR was 7% and the PDR was 34.2%. Polyp detection rate (PDR) is another indicator of colonoscopy quality. PDR is the number of colonoscopy containing polyps divided by the total number of exams. Numerous studies indicate that PDR can serve as a good surrogate for ADR [19, 20]. Regarding the comparison between the two groups, the results showed no significant difference in ADR, PDR and CDR. This confirms that when Kalinox is used as a primary sedation method, these quality criteria for colonoscopy are not reduced.
Limitations
In terms of limitations, we were missing a general anesthetic group to contrast with our Kalinox group during the same period of the crisis. Due to the small number of colonoscopies performed under general anesthesia at this time, this was difficult. Additionally, indications for colonoscopy ranged from screening colonoscopy to emergency therapeutic colonoscopy, and this may lead to bias in this study. We have not examined the comorbidities of patients, particularly surgical abdominal comorbidities that can complicate the colonoscopy and have an impact on the results. Furthermore, the procedures were performed by a variety of nurses and endoscopists with varied degrees of expertise, which could have an effect on the patient's general comfort level and, of course, the outcomes.
Conclusions
In times of health crisis, access to the operating room being limited, the Kalinox allowed us to continue screening for colorectal cancer by colonoscopy and to avoid a loss of opportunity for our patients. Our study revealed that the CIR, the detection rate of cancers, polyps and adenomas are not reduced when Kalinox is used as a first-line sedation method for colonoscopies. Female gender, age over 65 and insufficient intestinal preparation were associated with a lower CIR. No complications were found. This motivates us to implement this easier, more affordable sedation technique in our practice and to broaden the indications.
Abbreviations
Equimolar mixture of oxygen and nitrous oxide: MEOPA; Southern Ile de France hospital center: CHSF; Boston Bowel Preparation Scale: BBPS; Cecal intubation rate: CIR; Adenoma detection rate: ADR; Polyp detection rate: PDR; Cancer detection rate: CDR; Fecal Immunological Test: FIT; Statistical software Statistical Package for Social Sciences: SPSS; Standard deviations: SD
Acknowledgements
The sponsor was Centre Hospitalier Sud Francilien
Conflicts of Interest
The authors declare no conflict of interest.
References
1. Critères de qualité de la coloscopie. (2021). Accessed: January 12, 2022:
2. RECOMMANDATION DU CONSEIL du 2 décembre 2003 relative au dépistage du cancer. (2003). Accessed: February 11, 2022.
3. PROCEDURE D'UTILISATION DU MELANGE EQUIMOLAIRE PROTOXYDE D' AZOTE / OXYGENE. (MEOP A) . (2005). Accessed: February 11, 2022:
4. Omar M Aboumarzouk, Trisha Agarwal, Syed Aidil Hizman, et al. Nitrous oxide for colonoscopy. Cochrane Database Syst Rev. 2011, 8:CD008506. 10.1002/14651858.CD008506
5. Alexander R Robertson, Nicholas A Kennedy, James A Robertson, et al. Colonoscopy quality with Entonox®vs intravenous conscious sedation: 18608 colonoscopy retrospective study. World J Gastrointest Endosc. 2017; 9(9):471-479. 10.4253/wjge.v9.i9.471
6. S Welchman, S Cochrane, G Minto, et al. Systematic review: the use of nitrous oxide gas for lower gastrointestinal endoscopy. Aliment Pharmacol Ther. 2010; 32(3):324-33. 10.1111/j.1365-2036.2010.04359.x
7. Faisabilité des coloscopies avec analgésie par un mélange équimolaire d'oxygène et de protoxyde d'azote. Accessed: March 23, 2022.
8. Coloscopie sous MEOPA en immersion : une alternative à l’anesthésie générale. (2003). Accessed: March 27, 2022 .
9. La sédation par mélange équimolaire d’oxygène et de protoxyde d’azote n’est pas une alternative à l’anesthésie générale en endoscopie digestive.. Accessed: April 17, 2022.
10. A Akere, KO Akande. Cecal intubation rate during colonoscopy at a tertiary hospital in South-West Nigeria: How frequent and what affects completion rate?. Niger J Clin Pract. 2017; 20(3):303-306. 10.4103/1119-3077.187334
11. Hemant A Shah, Lawrence F Paszat, Refik Saskin, et al. Factors associated with incomplete colonoscopy: a population-based study. Gastroenterology. 2007; 132(7):2297-303. 10.1053/j.gastro.2007.03.032
12. G Dafnis, F Granath, L Påhlman, et al. Patient factors influencing the completion rate in colonoscopy. Dig Liver Dis. 2005; 37(2):113-8. 10.1016/j.dld.2004.09.015
13. Hong-Jun Park, Jin-Heon Hong, Hyun-Soo Kim, et al.Predictive factors affecting cecal intubation failure in colonoscopy trainees. MC Med Educ. 2013; 13:5. 10.1186/1472-6920-13-5
14. Brian P Saunders, Manabu Fukumoto, Steve Halligan, et al. Why is colonoscopy more difficult in women?. Gastrointest Endosc. 1996; 1016:0016-5107. 10.1016/s0016-5107(06)80113-6
15. Edwin J Lai, Audrey H. Calderwood, Gheorghe Doros et al: The Boston Bowel Preparation Scale: A valid and reliable instrument for colonoscopy-oriented research . Gastrointest Endosc. 2009; 69(3 Pt 2):620-625. 10.1016/j.gie.2008.05.057
16. Douglas A Corley, Christopher D Jensen, Amy R Marks, et al. Adenoma Detection Rate and Risk of Colorectal Cancer and Death. N Engl J Med. 2014; 370:1298-1306. 10.1056/NEJMoa1309086
17. Jae Young Jang, Hoon Jai Chun. Bowel preparations as quality indicators for colonoscopy . World J Gastroenterol. 2014; 20(11):2746-2750. 10.3748/wjg.v20.i11.2746
18. Philip S Schoenfeld, Jonathan Cohen. Quality indicators for colorectal cancer screening for colonoscopy. Tech Gastrointest Endosc. 2013; 15(2):59-68. 10.1016/j.tgie.2013.02.005
19. Leonardo Zorron Cheng Tao Pu, Gurfarmaan Singh, Khizar Rana, et al. Polyp Detection Rate as a Surrogate for Adenoma and Sessile Serrated Adenoma/Polyp Detection Rates. Gastrointest Tumors. 2020; 7(3):74-82. 10.1159/000505622
20. G Hoff, E Botteri, O Høie, et al. Polyp detection rates as quality indicator in clinical versus screening colonoscopy . Endosc Int Open. 2019; 7(2): E195-E202. 10.1055/a-0796-6477
Received: January 04, 2023;
Accepted: February 13, 2023;
Published: February 16, 2023.
To cite this article : Abboud R, Houist G, Lambare B, et al. Quality of Colonoscopies Under Kalinox during the COVID-19 Epidemic. British Journal of Gastroenterology. 2023; 5(1): 273-277. doi: 10.31488/bjg.1000135.
© Abboud R, et al. 2023.