
Research article / Open Access
DOI:10.31488/bjg.1000145
Randomized Single-Blind Clinical Trial Comparing Left Lateral Decubitus Position vs. Supine Position for Colonoscopies: A Multicenter Study
Dr. Roberto Ulises Cruz Neri*1,2, Fray Antonio Alcalde1, José Vicente Villada2, Dr. Athziri Buenrostro Fernandez1, Dr. Luis Antonio Ruiz Mares1, Dr. Carlos Humberto Sandoval Jimenez2, Dr. Francisco Javier Valadez Correa1, Dr. Jose Alberto Gonzalez Duarte1, Dr. Florisa Hernández Gómez1, Dr. Milton Miguel Salas Nuñez1, Dr. José Carlos Gomar González¹, Dr. Carolina Vázquez Iñiguez1, Dr. María Luisa López Ibañez1, Dr. Samantha Michelle Delgadillo Barajas¹, Dr. Alma Abigail Perez Diaz1S
1.Hospital Civil Antiguo, Colorectal Surgery Department , Mexico
2.Hospital General Regional No. 220 , Mexico
*Corresponding author: Dr. Roberto Ulises Cruz Neri, Specialty: Coloproctology, ORCID: 0000-0002-1034-9412; Tel: 3311946664; E-mail: robertocruzneri@gmail.com
Abstract
A multicenter study was conducted to determine the efficacy of the left lateral decubitus position (LLD) versus the supine position (SP) during colonoscopies. The study evaluated the time to reach the cecum, the percentage and time to intubate the ileocecal valve, the polyp detection rate, and the formation of loops requiring reduction maneuvers or position changes. A total of 144 patients were analyzed (40 at Hospital Civil Fray Antonio Alcalde and 104 at Hospital General Regional No. 220 "José Vicente Villada"), with an average age of 57.7 years (SD ±12.2). The overall cecal intubation rate was 99.3% (143/144), with no significant differences between positions. The time to reach the cecum was similar between groups (LLD: 528.5 ± 264.4 s vs. SP: 490.6 ± 308.0 s; p=0.47). It was observed that position changes were necessary in 33.33% of patients in the LLD group, compared to 31.82% in the SP group, although this difference was not statistically significant. The overall polyp detection rate was 20.7%, with rates of 21.27% in LLD and 30.43% in SP, without statistically significant differences. In conclusion, both positions proved to be safe and effective, with no relevant differences in intubation, times, or polyp detection. LLD was associated with fewer additional maneuvers, while SP showed a trend towards higher polyp detection. Additional studies with larger sample sizes are needed to confirm these findings and extrapolate them to other populations.
Keywords: Colonoscopy, supine position, left lateral decubitus position
Introduction
Currently, colonoscopy is one of the most widely used procedures for the study and treatment of patients with gastrointestinal conditions, including colorectal cancer and inflammatory bowel disease [1]. In the area of colorectal neoplasia, colonoscopy has three main functions: detecting the disease, preventing its development by detecting and removing potentially premalignant lesions, and providing a diagnosis of early-stage cancers [2]. In fact, more than 15 million colonoscopies are performed annually in the United States, and it is estimated that the procedure reduces the risk of death from colorectal cancer by more than 60% [3]. The efficacy of colonoscopy is crucial for conducting a precise examination of the entire colorectal mucosa, which is why the quality of the procedure has been a topic of study in recent years [2]. Among the various factors influencing the quality of colonoscopy is bowel preparation [5]. The position during colonoscopy is another factor that can influence its efficacy; traditionally, colonoscopy is initiated and completed, if no position changes occur, in the left lateral position. However, recent evidence suggests that the supine position could alleviate the disadvantages of the left lateral position by reducing the frequency of position changes and abdominal pressure, potentially resulting in easier insertion in the supine position compared to the left lateral position. However, few studies have evaluated the impact of the supine position during colonoscopy insertion [6].
Materials and Methods
A randomized single-blind clinical trial was conducted from August 1, 2024, to July 31, 2025, in patients scheduled for colonoscopy who were admitted to the Endoscopy and Coloproctology Service of Hospital Civil Fray Antonio Alcalde and Hospital General Regional No. 220 "José Vicente Villada." Eligible patients, according to established guidelines, were scheduled for colonoscopy and assigned a randomized number. Upon arrival for their appointment, they were informed about the clinical trial, and the informed consent was explained, including the purpose of the protocol, as well as the risks and benefits associated with the study. Once the consent was signed, patients were randomized to start the colonoscopy in the LLD or SP. All relevant information was recorded in a shared database between both sites. Subsequently, the database was cleaned and exported to the SPSS statistical package for data analysis, allowing for the development of conclusions.
Results
A total of 144 patients undergoing colonoscopy were analyzed, with 40 patients (27.6%) at Hospital Civil Fray Antonio Alcalde and 104 patients (71.7%) at Hospital General Regional No. 220 "José Vicente Villada." The average age was 57.7 years (SD ±12.2). Regarding the primary objective of the study, the overall cecal intubation rate was 99.3% (143/144), with no statistically significant differences when comparing the LLD and SP. The time to reach the cecum showed similar means between both positions (528.5 ± 264.4 seconds vs. 490.6 ± 308.0 seconds), with no significant differences (p = 0.47, 95% CI -112.01 – 117.01). Regarding comfort and additional maneuvers, which included loop formation and the need for rectification maneuvers, it was observed that in the LLD position, position changes were necessary in 33.33% of patients, while in the supine group, the percentage was 31.82%. These percentages suggest that, regardless of the institution, the need for repositioning is frequent and without statistical significance. In the analysis of polyp detection, the overall rate was 20.7% (Figure 1).
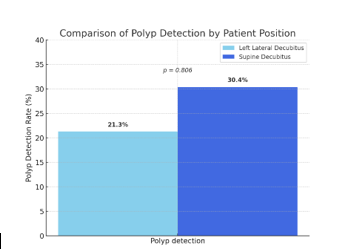
Figure 1:Comparison of Polyp Detection by Patient Position.
Discussion
Colonoscopy is the gold standard for the detection and prevention of colorectal cancer, allowing the identification of precursor lesions and their treatment in the same procedure. The quality of colonoscopy depends on factors such as bowel preparation, patient position, endoscopist experience, withdrawal time, and patient position during the examination [2].
The patient's position during colonoscopy has received increasing attention. The left lateral decubitus (LLD) position has been considered the traditional position due to its logistical ease and the comfort it provides to both the patient and the operator. However, the supine (SP) position has been proposed as an alternative with potential advantages in mucosal visualization, especially in the detection of adenomas and polyps [1].
This study compared the effectiveness of colonoscopy between the left lateral decubitus and supine positions in two hospital settings, each with a marked tendency towards one position compared to the other. In the Hospital Civil Fray Antonio Alcalde, the vast majority of procedures are performed in the left lateral position, while in the Hospital Regional No. 220 "José Vicente Villada," the usual position is supine. Therefore, the aim was to subject the different sites to use the non-habitual position and compare their results with those of the other hospital unit.
Firstly, the overall cecal intubation rate was 99.3%, confirming the high quality of the procedure in both institutions. When analyzed by groups, it was observed that the cecal intubation rate was 98.2% at HCFAA, while it was 100% at IMSS. This difference did not reach statistical significance, suggesting that the initial position does not compromise the efficacy of the procedure. However, it is noteworthy that the only case without cecal intubation was recorded at HCFAA, which could be attributed to technical variations between operators rather than the position itself, or to the patient's anatomical characteristics, as cecal intubation was not achieved despite changing positions [3].
Regarding cecal intubation time, the results were similar between positions, both at HCFAA and IMSS, with no significant differences. This partially contradicts the initial hypothesis favoring the supine position and aligns with literature reports describing that intubation time depends more on the endoscopist's practice and the patient's individual anatomy than on the initial position. The multicenter analysis did not stratify the results by gender, limiting direct comparison. This is relevant considering that female gender has been described as a predictor of greater difficulty in colonoscopy due to pelvic anatomy and greater colonic redundancy. This data opens the door to considering personalization of the initial position according to the patient's gender, something that has not been strongly reported in the literature [5].
An interesting finding was the need for position changes during the procedure. At HCFAA, changes were necessary in 33.33% of cases, while at IMSS, this proportion decreased to 31.82%. These percentages suggest that, regardless of the institution, the need for repositioning is frequent and relatively similar between scenarios, which could be more related to the anatomical variability of patients than to the initial position itself. However, contrasting with previous studies, LLD usually requires fewer additional maneuvers, which can be interpreted as a more agile procedure for the endoscopist.
It is undeniable, as established by the American Gastroenterological Association in its Clinical Practice Update on Strategies to Improve the Quality of Screening and Surveillance Colonoscopy, that the adenoma detection rate (ADR) is one of the best quality indicators in colonoscopy, and a high ADR correlates with a significant reduction in interval colorectal cancer and mortality [6].
Regarding the polyp detection rate, a different pattern was observed between hospitals. At HCFAA, the detection rate was 21.3%, while at IMSS, it was higher, reaching 30.4%. This trend is consistent with international studies suggesting that SP could offer better mucosal exposure, particularly in segments such as the ascending colon, where luminal collapse can hinder visualization in LLD. Although the difference was not significant, this trend could suggest that the supine position offers a slight advantage in lesion visualization, possibly because it facilitates colonoscope advancement in proximal segments and improves mucosal exposure (Figure 2 and 3).
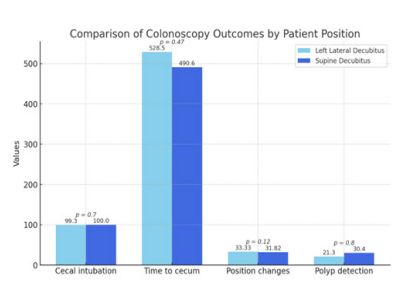
Figure 2:Comparison of Colonoscopy Outcomes by Patient Position.
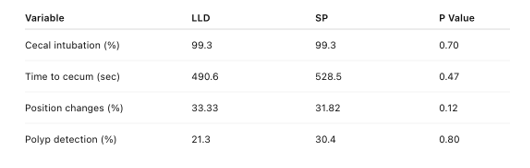
Figure 3:Comparison of cecal intubation, procedure time, position changes, and polyp detection between left lateral decubitus and supine positions.
However, it is also important to recognize that polyp detection depends on multiple factors, including bowel preparation quality, colonoscope withdrawal time, and endoscopist experience, so it cannot be attributed exclusively to the initial position.
Conclusions
The supine and left lateral decubitus positions did not show differences in terms of time to reach the cecum, polyp detection rate, and need for position changes. However, further studies are needed to extrapolate our findings to other populations.
Abbreviations
LLD: Left Lateral Decubitus; SP: Supine Position; HCFAA: Hospital Civil Fray Antonio Alcalde; IMSS: Mexican Social Security Institute; SPSS: Statistical Package for the Social Sciences
Acknowledgments
This protocol was conducted without sponsorship. The authors express their gratitude to the hospital units for their valuable collaboration and for allowing the execution of the study.
Conflict of Interest
The investigators declare no conflict of interest for conducting this study.
References
1. Greene A, Borgoankar M, Hodgkinson K, Garland C, Bacque L, Pace D. A randomized controlled trial comparing right and left lateral decubitus starting position on outcomes in colonoscopy. Surg Endosc. August 2020;34(8):3656-62.
2. Church J. Colonoscopy: what are we missing? Surg Oncol Clin N Am. January 2014;23(1):1-9.
3. Gangwani MK, Aziz A, Dahiya DS, Nawras M, Aziz M, Inamdar S. History of colonoscopy and technological advances: a narrative review. Transl Gastroenterol Hepatol. April 20, 2023;8:18.
4. Chokshi RV, Hovis CE, Hollander T, Early DS, Wang JS. Prevalence of missed adenomas in patients with inadequate bowel preparation on screening colonoscopy. Gastrointest Endosc. June 2012;75(6):1197-203.
5. Zhao S, Yang X, Meng Q, Wang S, Fang J, Qian W, et al. Impact of the supine position versus left horizontal position on colonoscopy insertion: a 2-center, randomized controlled trial. Gastrointest Endosc. June 2019;89(6):1193-1201.e1.
6. Zhao S, Yang X, Meng Q, Wang S, Fang J, Qian W, et al. Impact of the supine position versus left horizontal position on colonoscopy insertion: a 2-center, randomized controlled trial. Gastrointest Endosc. junio de 2019;89(6):1193-1201.e1.
Received: September 10, 2025;
Accepted: September 17, 2025;
Published: September 24, 2025.
To cite this article : Cruz Neri RU, Alcalde FA, Villada JV, Buenrostro Fernandez A, Ruiz Mares LA, Sandoval Jimenez CH, et al. Randomized single-blind clinical trial comparing left lateral decubitus position vs. supine position for colonoscopies: A multicenter study. Br J Gastroenterol. 2025;7(1):322-325. doi:10.31488/bjg.1000145.
© The Author(s) 2025. This is an open access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/).